Hip osteonecrosis
What is osteonecrosis?
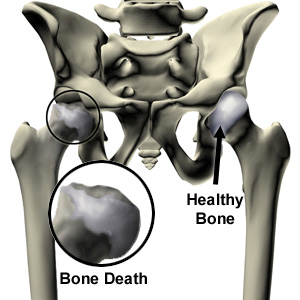
The bones in our body are like any other tissue; they require blood vessels to bring blood to the tissue to keep them functioning. Osteonecrosis occurs when the normal blood supply to the bones stops, and the bone can no longer regenerate and repair itself. The hip has a limited blood supply, with the blood vessels passing up the femoral neck into the femoral head. If these are damaged, osteonecrosis can set in and the femoral head starts to degenerate, starting in the areas that are subject to most wear and tear and pressure. The femoral head starts to crumble away and flatten, so that it no longer fits snugly into the socket, and osteoarthritis may then set in.
What causes it?
Anything that damages the blood vessels can cause osteonecrosis. Therefore a hip injury, a fracture of the femoral neck, or a hip dislocation can cause it. Environmental factors can raise the chances of you contracting osteonecrosis: alcoholism is linked to the development of osteonecrosis, as is exposing the body to high atmospheric pressure (thus divers and miners are more at risk). Taking high dosages of cortisone for a long time has also been linked to the development of osteonecrosis.
How does it feel?
The main symptom is pain. When you put weight through the hip, you may feel pain in your groin, your buttocks or down the front of your thigh. As the condition develops, the joint may become stiff and the pain almost constant.
Diagnosis
Your doctor will ask you about your medical history and lifestyle, and he will make a physical examination. He will ask for X-rays of your hip to show the shape and condition of the bones. In the early stages of osteonecrosis, an X-ray may not be conclusive, so your doctor may ask you to have a bone scan or an MRI (magnetic resonance imaging) scan.
Treatment – conservative
Your doctor may ask you to reduce or remove the weight you put through your hip, so you will need crutches for walking. He will also ask you to make changes in your lifestyle if necessary, such as stopping smoking or drinking alcohol. He may also prescribe any of the following treatments:
- shock wave therapy
- hyperbaric oxygen therapy
- medication (such as biphosphonates)
Treatment – surgical
In the early stages, your surgeon will perform the following procedure:
Core Decompression: your surgeon will make 2-3cm incision on the side of your hip. He will drill a tunnel up the femoral neck and into the femoral head, removing a plug of bone. This releases the liquids and reduces the pressure inside the bone. In some cases, he will inject growth factors into the tunnel to encourage bone re-growth, and/or re-insert the plug of bone.
For more advanced cases, one of the following procedures will be used:
Hip Osteotomy: your surgeon will make a 10-12cm lateral incision, through which he will cut through the femoral neck. He will rotate the femoral head, so that a healthy area of bone is now taking the wear and tear, and re-attach it to the femur using a metal plate. This procedure is used mainly for young, patients.
Total Hip Replacement: A hip prosthesis is made up of 2 parts: the acetabular component which replaces the socket, made of a metal cup lined with a plastic or ceramic liner; and the femoral component which is a metal ball and stem (or sometimes a ceramic ball and metal stem), and replaces the femoral head.
The surgeon will make a 10-12cm incision on the outside of the hip. Then he will shape the acetabulum to fit the socket-shaped acetabular component, removing all the damaged cartilage and bone. Next he will remove the femoral head, and make a tunnel down the femur to house the stem of the femoral component. He will then fit the components into place, fixing them with bone cement if he is using a cemented prosthesis. Your surgeon will then align the joint and ensure that the leg rotates and moves correctly. After surgery, you should have a correctly aligned hip and a full range of motion.
Femoral Resurfacing: your surgeon will make a 10-12cm lateral incision through which he will smooth and shape the femoral head, and the acetabulum so that they are the right shape to fit the artificial hip components. He will then place a metal cover or cap over the top of the femoral head, fixing it with bone cement, and fix the acetabular component into the acetabulum. Again, this procedure is used for younger patients
Rehabilitation after surgery
Core decompression: you should be able to go home with crutches the same day as your operation, and you will need to use them for about 4 weeks, gradually increasing the amount of weight you put through your leg. You will be given exercises to do at home, although after a few weeks you should start a physiotherapy programme to regain a full range of hip movement and rebuild your muscles.
Hip osteotomy: you will need to use crutches for 2 months after the operation, putting no weight at all on your leg for the first 45 days. You will be given exercises to keep the muscles in your leg moving during this time. Once you can start to put weight on your leg, you will be given a more strenuous physiotherapy programme to build up muscle strength and range of movement.
Femoral Resurfacing: you will be in hospital for 4-6 days after the operation and you will need to walk with crutches for the first 6 weeks, moderating the amount of weight you put through your hip. You will start physiotherapy immediately after the operation, initially to learn how to do simple activities safely, and to start moving your leg. Once you are at home, you will follow a physiotherapy programme to rebuild your leg and hip muscles, regain your range of movement and develop your balance and the control of your hip.
Hip Replacement: you will be in hospital for 1-2 weeks after surgery. During this time a physiotherapist will have shown you what movements you can and can’t do, and how to perform ordinary activities safely. You will also be given exercises to start moving your hip immediately, and then, once you have left hospital, you will have to follow a physiotherapy programme to rebuild your muscles and regain hip functionality. You will need to walk with crutches for the first 6 weeks, gradually increasing the amount of weight you put on the operated leg. You will also have to sleep with a pillow between your legs for the first month, and use a raised toilet seat for 2 months.