Meniscus Tears
What is a meniscus tear ?
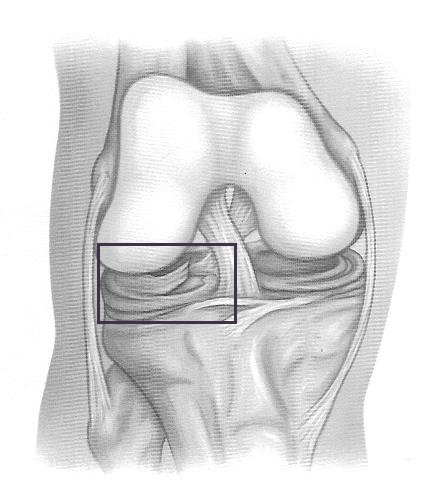
The two menisci (singular – meniscus) are made of a rubbery cartilage that acts like a shock absorber in the knee. They are wedge-shaped and sit on the top end of the tibia, distributing the bodyweight transmitted down the femur. They also help stabilise the knee by forming a kind of cup for the femur – without them the round femur head would slide on top of the flat surface of the tibia. If a piece of meniscus tissue is torn, it can move around in the knee, getting trapped between the bones of the joint causing irritation, swelling, locking, or sometimes a sensation of ‘giving way’. If the tear is not treated, it can rub against the articular cartilage causing the surface to become worn which can lead eventually to osteoarthritis.
What causes it?
Meniscus tears are usually the result of a forceful twisting or pivoting motion in the knee, and so are commonly incurred whilst playing sport. However, as the meniscus weakens with age, a fairly minor injury – even standing up after squatting – can cause a meniscus tear. Often in older patients there may not even be a specific incident that has caused the tear, just a general degeneration in the meniscus which has made it frayed.
How does it feel?
The most common symptom is pain, whether located specifically at the point of the damaged meniscus, or more vaguely across the knee. The knee may swell or lock if a piece of the menuiscus has torn free and is caught in the “hinge”mechanism of the knee.
Diagnosis
An analysis of your medical history and a physical examination should enable the doctor to make a diagnosis (the doctor will determine the location of pain and see if the knee locks or makes noises when it moves). If these do not produce a clear diagnosis, the doctor may suggest an MRI (Magnetic Resonance Imaging) scan which clearly shows ligament/meniscus damage.
X-rays will not show a torn meniscus, but will show if there is bone damage.
Treatment – conservative
The immediate priorities with a torn meniscus are to decrease pain and swelling in the knee and so the doctor will prescribe rest and anti-inflammatory medication. You may need to use crutches until you can walk without a limp.
Treatment – surgical
If symptoms continue after conservative treatment, arthroscopic surgery will probably be suggested to either remove or repair the torn part of the meniscus. Arthroscopic meniscal surgery: is an operation that involves inserting a miniature fibre-optic TV camera into the knee joint, allowing the orthopaedic surgeon to see the condition of the soft tissues. The surgeon will perform either a Partial Meniscectomy (removing only the damaged piece of meniscus and any debris in the joint) or a Meniscal Repair (the edges of the tear are sewn or anchored together). Only if the entire meniscus is damaged beyond repair is the whole meniscus removed. In certain cases, a transplant (called an allograft) may be made if there is a suitable donor.
Rehabilitation after surgery
Treatment will depend on the type of operation performed. After a partial meniscectomy, your surgeon may instruct you to place a comfortable amount of weight on your operated leg using crutches. After a meniscal repair, however, you will be instructed to restrict the range of movement, possibly with a knee brace, and to put only minimal or no weight on their foot when standing or walking for up to six weeks. Physiotherapy exercises may also be prescribed by your surgeon for 6-8 weeks after the operation.